For California Native medical students, practicing cultural humility is PRIME

By shaylyn martos
Desirae Barragan hugs her program co-directors on stage at the Blue Lake Rancheria Casino, smiling into a sea of faces and a swell of cheers. Across her shoulders – and those of her fellow graduates of the Huwighurruk Tribal Health Program – drapes a blue “Warrior Blanket” emblazoned with golden stars across her back, designed by artist Dante Biss-Grayson (Osage) for Eighth Generation in collaboration with Sky Eagle.
“I often have the isolated experience of being the only California Native. But in that room, I think I really felt the pride to acknowledge my roots,” Barragan (Gabrieleno Band of Mission Indians of Southern California) said.
It was graduation day for all the American Indian students at Cal Poly Humboldt, and there was no limit on how many friends and family could attend. Barragan remembers shaking hands with elders, community members and leaders who told her, “We would love to have you back up here as a provider.”
The California State Health Assessment estimates 7 million Californians live in health professional shortage areas, and Black, Latinx, American Indian and Alaskan Native (AI/AN) people are the most at risk. Currently, AI/AN life expectancy is 67.8 years, nearly a decade below the national average.
Not only are American Indian physicians expected to be experts in Native healthcare, some clinics offer services to all regardless of tribal affiliation. And with the current administration’s ongoing restructuring of the Department of Health and Human Services (HHS), more cuts to tribal health programs and Medicaid are on the horizon.
For minority students, the biggest barriers to becoming physicians occur long before they apply – systemic challenges disrupt access to safe housing, nutritional food and mental health care. About 50% of Native American students who apply to medical school are not admitted, and 43% of those never apply again.
Dr. Alec Calac, PhD (Pauma Band of Luiseño Indians) is an MD candidate at UCSD who helped establish their tribal-focused medical program: Transforming Indigenous Doctor Education.
“We are so poorly represented in health professional education, yet our communities often face the highest burden of disease and disparities across the board,” Calac said. “The literature shows people from these backgrounds are more likely to go back to their own communities and practice and stay there.”
In Arcata, Desirae Barragan shadowed tribal physicians, worked on bolstering her MCAT score (a test necessary for medical school admission), and witnessed ceremonies for Northern California tribal members blending conventional medicine and Indigenous healing.
After a gap year, which included organizing with the Portland-based Native Youth advocacy group We Are Healers, Barragan will join the UC Davis’ Tribal Health Program in Medical Education (PRIME) this fall.
URiM Students Rooted in Community:
Data from the Association of American Medical Colleges (AAMC) in 2025 shows that medical school enrollment is at an all-time high, approaching nearly 100,000 students nationwide. The AAMC coined the acronym URiM to mean students who identify with race or ethnic categories “underrepresented in medicine.”
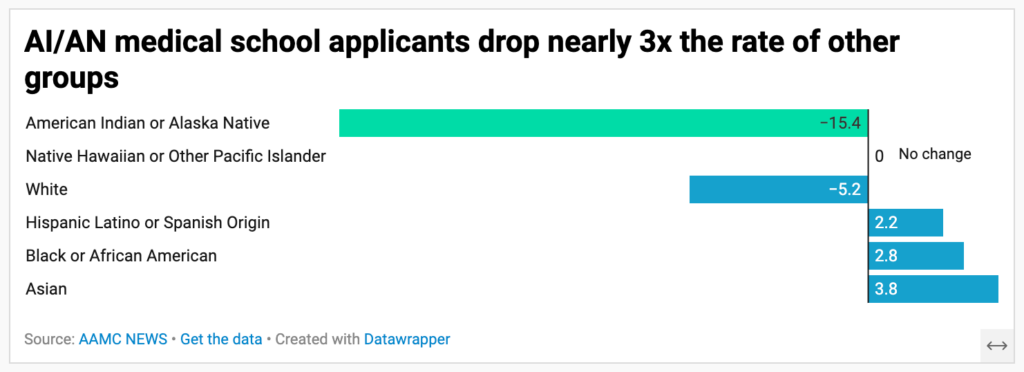
After a decade-long increase, the number of first-year URiM students fell in 2025, despite the number of Black and Hispanic or Latinx applicants rising. But AI/AN applicants and matriculants (meaning students that enter a university) defied that trend, dropping 15.4% and 22.1% respectively.
While underrepresented in medical schools, minority physician residents are more likely to practice in disadvantaged areas and in primary care settings.
UCSD MD candidate Dr. Alec Calac co-authored a 2024 analysis published in the Journal of the National Medical Association, which crunched over four years of data on minority groups in 34 specialties from 2019-2023. The authors found that AI/AN, Native Hawaiian, Black and Hispanic residents had higher odds for choosing family medicine, preventative medicine or psychiatry.
Calac acknowledges that a major difference for URiM students and minority physicians is that they’re often not seeking training for individual advancement, but they are rooted in community. “Because they’ve lived through the challenges that they’re trying to address, with their health professional training now they’re in a position where they can work to affect positive change,” Calac said.
Barragan’s grandmother Marylou Gonzalez Gomez (Gabrieleno Band of Mission Indians, San Gabriel) said she feels blessed that her granddaughter will be starting medical school soon, and that seeing Barragan help other people, especially their Native community, makes her very proud.
“In my culture, family and relationships are very important. What matters most to me is having a close bond with my doctors so they truly know who I am and understand my health concerns,” Gonzalez Gomez said. “It’s also important that my Native identity and traditions are honored and respected in my care.”
It’s hard for many Native Californian tribal communities to find translation services while seeking health care. It’s particularly challenging for the Kumeyaay people, whose territory spans north and south of the U.S.-Mexico border.
“The rights that they have as Indigenous peoples are very different between the U.S. and Mexico, simply because of a border that crosses their traditional lands,” Calac said. “They’re still the same people, they have the same culture, the same language, but they have very different ways in which they navigate their health systems.”
Despite being part of the Kumeyaay Nation, tribal members in Mexico are not considered “American Indian” by the U.S. government and do not have the same access to resources, or the privilege to travel freely for ceremonial healing practices. As a spokesperson for the Kumeyaay Heritage Preservation Council stated: “The Border Wall keeps us from continuing ancient and sacred ceremonies. It not only divides our nation, but it divides Kumeyaay families.”
Calac said he hopes the programs at UCSD and UC Davis set the standard for prioritizing tribal-focused learning starting from K-12th grade and undergraduate education.
“The legacy of these PRIME programs is that we will really train a workforce of California Indian physicians,” Calac said. “And I think that’s the dream that will be realized in the next generation.”
Carving the Huwighurruk Pathway:
The tribal-focused medical education programs at UCSD, UC Davis and Cal Poly Humboldt are attempting to recruit, retain and train a physician workforce that understands tribal communities’ distrust of Western medical systems and honors Indigenous sovereignty.
Antoinette Martinez (Chumash) is the curriculum lead for the UC Davis Tribal Health PRIME (THP) and co-director of the Huwighurruk (hee-way-gou-duck) program.
“We have had innumerable traumas as American Indians with colonization,” Martinez said, “And we know the effects of that which are being shown in epigenetics and historical trauma.”
It’s that legacy these programs are working against. To expand the pipeline of Native applicants into medicine, Martinez and UC Davis partnered with Cal Poly Humboldt to launch Huwighurruk (a Wiyot word meaning plants, grass, leaves and medicine) in 2024, with support from the Wy’east Medicine pathway based out of Oregon Health Sciences University in Portland.

The first cohort of Huwighurruk Tribal Health Program visits Dr. Walt Lara and Dr. Kishan Lara Cooper at Chahpekw O’ Ket’-toh “Stone Lagoon” during their orientation week. Courtesy of Antoinette Martinez
The Huwighurruk program functions as a pipeline – similar to college prep programs that provide hands-on tutoring, mentoring and application support to students facing structural barriers to high education. Those who complete the one-year post-baccalaureate program receive a conditional admission to the THP, effectively guaranteeing four of the six spots will be filled each year.
The remaining spots are harder to fill because the barriers to even applying to medical school — from MCAT scores to prerequisites, and GPA requirements — are disproportionately difficult for Native students.
“We have a higher than average risk for dropping out of medical school,” Martinez said. “Our students need support throughout to help them make it to the end.” She shared that when students leave their tribal lands and travel far for medical school, they often end up staying where they studied.
The UC Davis programs are place-based, where Northern California tribes benefit from having Native medical students in their communities. Students gain hands-on clinical experience working directly in Indian Health Service clinics and through the Association of American Indian Physicians network, across urban, tribal and rural settings.
Martinez’s goal is for students to understand the need to collaborate and cultivate relationships with tribal communities in California to help improve health overall – hoping that at least some of them decide to stay in the state, whether with their own tribal communities or others.
Tribal Health and Cultural Humility:
While other minority medical students are focused on culturally competent care, Martinez uses a different term for a Native context: cultural humility.
“I’m not a big fan of the word culturally competent, because it means that somebody out there is an expert on everything on our tribes and communities,” she said. “In the spirit of learning, we want cultural humility, so that people understand that we don’t know. And even within one tribe with different families, you’re going to hear different stories and practices that were passed down through generations.”
Desirae Barragan learned this first hand while shadowing with the Huwighurruk program. “I saw more non-native patients in some of these clinics than I did Native patients. And depending on the specific tribe that has a tribal clinic – either on their reservation lands, or if they’re in the IHS system – it really fluctuates on what type of patients you see and who’s prioritized,” Barragan said.
Data from the HHS shows that in the fiscal year 2024, nearly 200,000 California residents were actively receiving care in IHS clinics. Of those patients, 54% were classified as non-Indian and 46% were Indian. But, the ratio changes for each service area. In Yurok territory, including Arcata, 93% of the active patients using United Indian Health Services were Native.
Growing up, Barragan remembers that her family would drive an hour and a half to visit the American Indian Health & Services in Santa Barbara. She knew her Grandma preferred IHS, so she didn’t question it.
{kind=link}
“I value being able to have my daughter or another family member accompany me to my appointments, because in our culture we support one another and make decisions together,” said Gonzalez Gomez. “Having my family present helps me feel safe, respected and understood when it comes to my healthcare.”
Now Barragan was seeing things from the other perspective, considering the sacrifices different patients would make and how she could best support them.
“I was seeing some of the patients up in Humboldt County. They needed specialty care, and they had to drive all the way down to San Francisco for six hours,” Barragan said. “Seeing those different disparities made me think, maybe I’ll be the first physician in my tribe, but also maybe the first to pursue an additional specialty.”
Fostering Community:
Many prospective Native medical students come from areas where infrastructure for education and mentorship are largely absent, so it’s even more important for them to foster connection with others for support.
Emma Grellinger (Stockbridge-Munsee/Oneida) is the President of the Association of Native American Medical Students (ANAMS) and a graduating senior at the UCSF School of Medicine. Grellinger grew up knowing she wanted to be a physician, because she had a great role model – her mom.
“I mean pretty much have known I wanted to be a doctor my whole life, and largely inspired by my mom,” Grellinger said. “There’s a lot of steps along the way that kind of test you, like, is this really the right field for me? But at the end of the day, I think it’s a career where you always know that you’re doing something good for the world.”

ANAMS President Emma Grellinger (standing right) tables for the Native American Health Alliance for UCSF. Courtesy of Emma Grellinger
Grellinger chose UCSF because of its diverse patient pool – which includes the San Francisco General Hospital and their free clinic for asylum seekers – but she was disappointed by the lack of Native representation. She is only one of two Native students in her cohort, and one of eight in the med school overall.
Since attending the Association of American Indian Physicians conference in her second year of med school, Grellinger has gotten deeper and deeper into organizing her fellow students, including starting a summer camp at UCSF for American Indian youth each year focused on medicine, science, technology, engineering and math (STEM) research, and law.
Grellinger’s undergraduate degree was paid for by her tribe; she also received a privately funded scholarship for UCSF given to federally recognized tribal members who identify as female. But there are limitations to federal and state funding. In California alone, there are 109 federally recognized tribes and 55 that remain unrecognized — nationally, the full count of unrecognized tribes is unknown.
A 2022 San Francisco Public Press request for records listing all non-federally recognized tribes was denied by the Department of the Interior. For Native students hailing from unrecognized tribes, this bureaucratic uncertainty has consequences: they are locked out of the federal and tribal funding that makes medical school financially possible for many of their peers.
“As we go further and further in generations, it’s just not sustainable for all of us to be like 25% from our tribe,” Grellinger said. “It really burdens those people unfairly who are not eligible for these scholarships.”
Native medical students can feel pressure to pursue primary care — the less competitive and more community-facing path. But without Native specialists, patients who need that level of care will almost certainly be treated by someone with no connection to their people or culture.
Grellinger is forging her own path and is currently applying for residencies in orthopedic surgery; she will receive her own blanket of knowledge from UCSF when she graduates this May.
“There’s a huge primary care shortage across the entire country, certainly in Indian Country, we don’t have enough primary care doctors. But I’m a pretty firm believer that we need people to do everything,” she said. “Nothing you choose to do in medicine is wrong. There’s always going to be a need for you in your community, no matter what.”
This story was produced for the 2026 Ethnic Media Collaborative with support from the Center for Health Journalism at USC.
shaylyn martos is a California Local News Fellow with the UC Berkeley Graduate School of Journalism.